
Long-term exposure to air pollution has been linked to an increased risk of dying from COVID-19 and, for the first time, a study has estimated the proportion of deaths from the coronavirus that could be attributed to the exacerbating effects of air pollution for every country in the world.
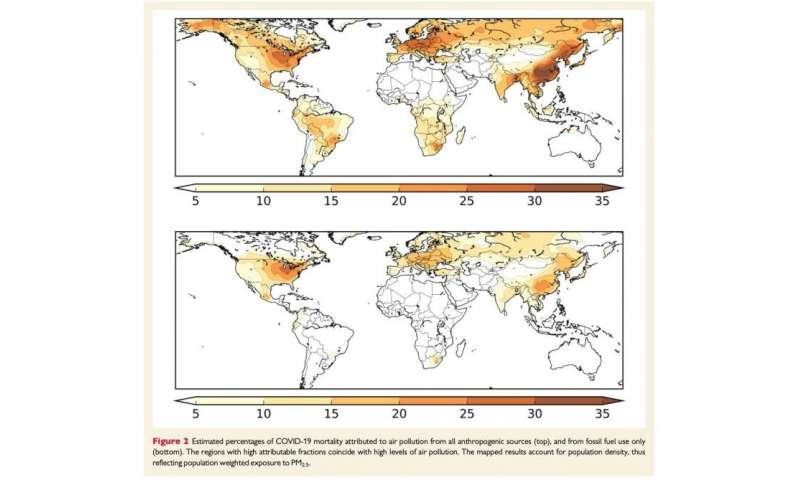
The study, published in Cardiovascular Research today, estimated that about 15% of deaths worldwide from COVID-19 could be attributed to long-term exposure to air pollution. In Europe the proportion was about 19%, in North America it was 17%, and in East Asia about 27%.
In their CVR paper, the researchers write that these proportions are an estimate of “the fraction of COVID-19 deaths that could be avoided if the population were exposed to lower counterfactual air pollution levels without fossil fuel-related and other anthropogenic [caused by humans] emissions”.
They add that this “attributable fraction does not imply a direct cause-effect relationship between air pollution and COVID-19 mortality (although it is possible). Instead it refers to relationships between two, direct and indirect, i.e. by aggravating co-morbidities [other health conditions] that could lead to fatal health outcomes of the virus infection”.
The research team includes Professor Jos Lelieveld, of the Max Planck Institute for Chemistry, Mainz, Germany, and the Cyprus Institute Nicosia, Cyprus, Professor Thomas Münzel, from the University Medical Center of the Johannes Gutenberg University, Mainz, and the German Center for Cardiovascular Research, Mainz, and Dr. Andrea Pozzer, from the Max Planck Institute for Chemistry.
The researchers used epidemiological data from previous US and Chinese studies of air pollution and COVID-19 and the SARS outbreak in 2003, supported by additional data from Italy. They combined this with satellite data showing global exposure to polluting fine particles known as ‘particulate matter’ that are less than or equal to 2.5 microns in diameter (known as PM2.5), information on atmospheric conditions and ground-based pollution monitoring networks, to create a model to calculate the fraction of coronavirus deaths that could be attributable to long-term exposure to PM2.5. The results are based on epidemiological data collected up the third week in June 2020 and the researchers say a comprehensive evaluation will need to follow after the pandemic has subsided.
Estimates for individual countries show, for example, that air pollution contributed to 29% of coronavirus deaths in the Czech Republic, 27% in China, 26% in Germany, 22% in Switzerland, 21% in Belgium, 19% in The Netherlands, 18% in France, 16% in Sweden, 15% in Italy, 14% in the UK, 12% in Brazil, 11% in Portugal, 8% in the Republic of Ireland, 6% in Israel, 3% in Australia and just 1% in New Zealand.
Prof. Jos Lelieveld said: “Since the numbers of deaths from COVID-19 are increasing all the time, it’s not possible to give exact or final numbers of COVID-19 deaths per country that can be attributed to air pollution. However, as an example, in the UK there have been over 44,000 coronavirus deaths and we estimate that the fraction attributable to air pollution is 14%, meaning that more than 6,100 deaths could be attributed to air pollution. In the U.S., more than 220,000 COVID deaths with a fraction of 18% yields about 40,000 deaths attributable to air pollution.”
Prof. Münzel said: “When people inhale polluted air, the very small polluting particles, the PM2.5, migrate from the lungs to the blood and blood vessels, causing inflammation and severe oxidative stress, which is an imbalance between free radicals and oxidants in the body that normally repair damage to cells. This causes damage to the inner lining of arteries, the endothelium, and leads to the narrowing and stiffening of the arteries. The COVID-19 virus also enters the body via the lungs, causing similar damage to blood vessels, and it is now considered to be an endothelial disease.
“If both long-term exposure to air pollution and infection with the COVID-19 virus come together then we have an additive adverse effect on health, particularly with respect to the heart and blood vessels, which leads to greater vulnerability and less resilience to COVID-19. If you already have heart disease, then air pollution and coronavirus infection will cause trouble that can lead to heart attacks, heart failure and stroke.”
Referring to previous work that suggests that the fine particulates in air pollution may prolong the atmospheric lifetime of infectious viruses and help them to infect more people [2], Prof. Lelieveld said: “It’s likely that particulate matter plays a role in ‘super-spreading events’ by favouring transmission.”
Prof. Münzel added: “Particulate matter seems to increase the activity of a receptor on cell surfaces, called ACE-2, that is known to be involved in the way COVID-19 infects cells. So we have a ‘double hit’: air pollution damages the lungs and increases the activity of ACE-2, which in turn leads to enhanced uptake of the virus by the lungs and probably by the blood vessels and the heart.”
In their paper, the authors conclude: “Our results suggest the potential for substantial benefits from reducing air pollution exposure, even at relatively low PM2.5 levels. . . . A lesson from our environmental perspective of the COVID-19 pandemic is that the quest for effective policies to reduce anthropogenic emissions, which cause both air pollution and climate change, needs to be accelerated. The pandemic ends with the vaccination of the population or with herd immunity through extensive infection of the population. However, there are no vaccines against poor air quality and climate change. The remedy is to mitigate emissions. The transition to a green economy with clean, renewable energy sources will further both environmental and public health locally through improved air quality and globally by limiting climate change.”
The study is also the first of its kind to distinguish between fossil fuel-related and other human-made sources of air pollution.
Source: Read Full Article