
Where to buy generic soloxine coupons no prescription
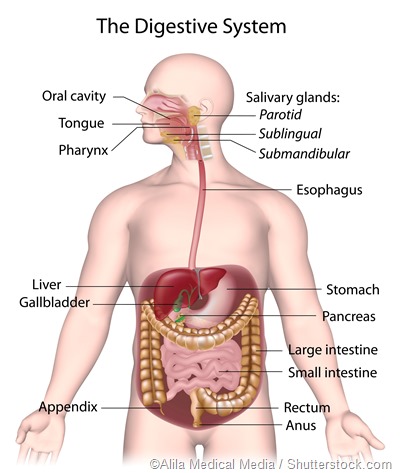
The gastrointestinal (GI) tract begins in the mouth and works its way down the esophagus, through the stomach, small and large intestines and rectum, before terminating at the anus. Bleeding or hemorrhaging anywhere along this pathway may be acute or chronic and can be due to a host of factors.
The key symptoms are hematemesis (vomiting blood) and/ or melena (black stool, i.e., blood in stool). Accompanying symptoms vary, but may include epigastric and diffuse abdominal pain, pale skin, shortness of breath, and alterations of consciousness.
Bleeding within the GI tractis itself not a disease, but rather a symptom of a disease. This bleeding may be divided into upper and lower GI bleeding. The upper GI tract consists of the oral cavity, esophagus, stomach, and the first part of the small intestine – the duodenum. The lower GI tract constitutes all other parts of the GI tract beginning at the midsection of the small intestine – the jejunum to the anus.
The major causes of upper GI bleeding include: esophageal varices, gastritis, peptic ulcers, inflammation, and cancer. The most common conditions associated with lower GI bleeding include diverticulitis (diverticular disease), infections, polyps, inflammatory bowel disease, hemorrhoids, anal fissures and cancer.
Upper gastrointestinal bleeding
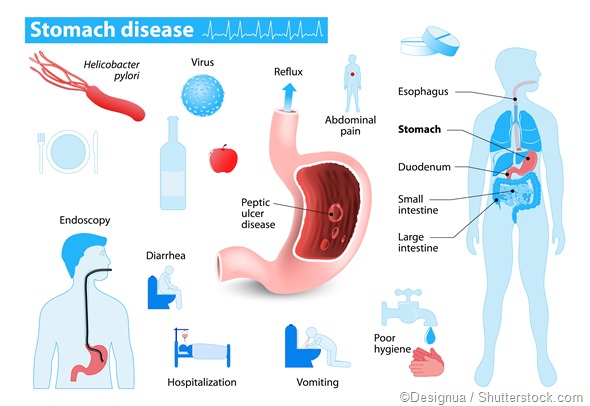
Bleeds from the upper GI tract are significant causes of morbidity and mortality and are much more common than lower GI bleeds. Important to note is that mortality associated with upper GI bleeds are often as a result of comorbidities rather than the actual bleeding itself. Peptic ulcers are the most common cause of upper GI bleeding.
Peptic ulcer disease (PUD) accounts for up to 40% of cases and those at particularly high risk for PUD include alcoholics, patients on extensive NSAIDs, and those with chronic renal failure. PUD has been strongly linked to infection with Helicobacter pylori.
This bacterium is responsible for the destruction of protective mechanisms in the stomach and duodenum leading to damage by stomach acid that would otherwise not be a problem. These ulcers are found more commonly in the duodenum than in the stomach, although both locations present with equal incidences of bleeding.
Esophageal inflammation and erosive esophagitis and erosive gastritis represent the second most common causes of upper GI bleeding. Acid reflux is the most common cause of inflammation of the esophagus. Esophageal varices (abnormally dilated vessels) are typically seen in patients with portal hypertension and chronic liver disease and these patients are at an increased risk for hemorrhage.
In addition to these, vomiting, due to force, can cause ruptures in the esophagus (Boerhaave syndrome) and resultant upper GI bleeding. Patients in shock due to trauma, sepsis, or organ failure can also have upper GI bleeds as a result of erosions occurring in the presence of decreased blood flow and altered acidity of the gastric lumen.
Lower gastrointestinal bleeding
Lower GI bleeding accounts for up to one third of all GI hemorrhages and is a very frequent cause of admission to the hospital due to its association with increased morbidity and mortality. Bleeding in this segment of the GI tract may be classified into 3 categories: massive bleeding, moderate bleeding, and occult bleeding.
As implied, massive bleeding is a potentially life-threatening condition that requires immediate blood transfusions. Occult bleeding is seen most often with colorectal cancer and patients typically present with iron deficiency anemia.
Approximately 6 in every 10 lower GI bleeds are due to diverticular disease, which includes diverticulitis of the small intestine and of the colon. Constipation, a lack of fiber in the diet, advancing age, and the use of drugs such as aspirin and NASIDs are all risk factors for diverticular disease.
Small vascular malformation of the GI (angiodysplasia), often in the ascending colon, associated with conditions such as chronic renal failure, may also give rise to hemorrhaging. However, it is less intense than diverticular disease, since the bleeding is from veins and/ or capillaries.
Inflammatory bowel diseases, such as Chron’s disease, ulcerative colitis, and non-infectious gastroenteritis account for just over a tenth of lower GI hemorrhages, while neoplasms and benign anorectal diseases such as hemorrhoids and anal fissures account for 20%.
These result in bleeding due to destruction of the bowel mucosa. Some bacterial GI infections also cause hemorrhaging due to the same mechanism. Other causes of lower GI bleeds include opportunistic infections associated with HIV, such as lymphoma, CMV-colitis, and Kaposi sarcoma.
Sources
- https://www.nlm.nih.gov/medlineplus/gastrointestinalbleeding.html
- www.mayoclinic.org/…/con-20035736
- http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4231512/
Further Reading
- All Gastrointestinal Bleeding Content
- What is Gastrointestinal Bleeding?
- Gastrointestinal Bleeding Treatment
- Gastrointestinal Bleeding Symptoms
Last Updated: Feb 26, 2019

Written by
Dr. Damien Jonas Wilson
Dr. Damien Jonas Wilson is a medical doctor from St. Martin in the Carribean. He was awarded his Medical Degree (MD) from the University of Zagreb Teaching Hospital. His training in general medicine and surgery compliments his degree in biomolecular engineering (BASc.Eng.) from Utrecht, the Netherlands. During this degree, he completed a dissertation in the field of oncology at the Harvard Medical School/ Massachusetts General Hospital. Dr. Wilson currently works in the UK as a medical practitioner.
Source: Read Full Article